
Suicide in Kenya presents a deeply troubling and complex public health reality shaped by economic hardship, mental health challenges, substance abuse, and widening social pressures that continue to intensify across both rural and urban landscapes.
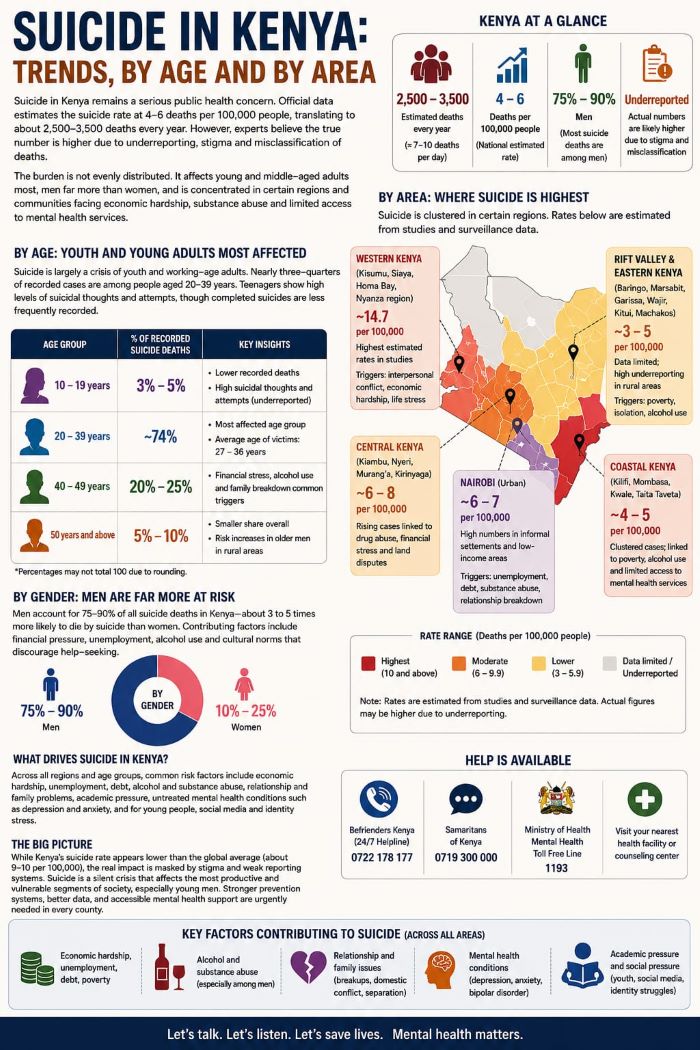
Although official estimates place the national suicide rate at approximately 4 to 6 deaths per 100,000 people — translating to roughly 2,500 to 3,500 deaths annually — experts consistently caution that the true burden is likely higher.
This is due to stigma surrounding mental illness, cultural silence around suicide, misclassification of deaths, and gaps in reporting systems affecting both densely populated cities and remote rural regions.
What emerges from available data is not a uniform national pattern, but a fragmented crisis marked by sharp demographic and geographic inequalities.
Suicide in Kenya is not evenly distributed. Instead, it clusters in certain age groups, regions, and social environments where economic pressure, emotional distress, and limited access to mental health care converge.
Young adults remain the most affected group
The most affected population is young and middle-aged adults between 20 and 39 years, who account for nearly three-quarters of all recorded suicide cases.
This is the most economically active stage of life, often associated with career development, family formation, financial responsibility, and social expectations. Yet it is also the stage where pressure appears most intense.
Many victims fall within the late twenties to mid-thirties age bracket, reflecting a painful intersection between rising expectations and limited opportunities.
Unemployment, unstable income, debt, and family obligations often combine to create prolonged psychological strain that, in many cases, goes unaddressed.
Teenagers form a smaller share of recorded suicide deaths — roughly 3 to 5 percent — but their situation reveals a deeper and more hidden crisis.
In urban environments such as Nairobi, studies have shown that a significant number of adolescents experience suicidal thoughts, with a worrying proportion reporting attempts.
This contrast between low official death records and high levels of psychological distress suggests that youth mental health challenges are widely underreported and often unrecognised.
Academic pressure, family conflict, bullying, identity struggles, and increasing exposure to social media comparisons all contribute to emotional vulnerability among teenagers.
Men account for the majority of suicide deaths
Gender differences in suicide patterns in Kenya remain both stark and persistent.
Men account for approximately 75 to 90 percent of all suicide deaths, making them significantly more likely to die by suicide than women.
This pattern is closely tied to structural and cultural factors. Men are often expected to be providers, resilient, and emotionally restrained, leaving little room for open expression of distress.
Economic pressures such as unemployment, the rising cost of living, debt, and financial instability further deepen vulnerability.
Alcohol and substance abuse also play a major role in many cases, often acting as both a coping mechanism and a risk multiplier.
Women, although recording fewer completed suicides, still experience significant psychological distress.
Their risk factors tend to differ, with relationship breakdowns, domestic violence, caregiving burdens, and economic dependence being more prominent.
In many cases, women experience prolonged emotional suffering without adequate access to support systems or safe reporting channels.
The gender gap in suicide deaths, therefore, does not reflect an absence of distress, but rather differences in expression, methods, and social conditions.
Regional patterns reveal deeper inequalities
Geographically, suicide in Kenya shows strong clustering patterns reflecting underlying inequalities in development, healthcare access, and social stability.
In coastal regions, particularly Kilifi, surveillance systems have recorded steady suicide cases with estimated rates of around 4 to 5 per 100,000 annually.
These cases are frequently associated with poverty, substance use, unemployment, and limited availability of mental health services.
The combination of economic marginalisation and healthcare gaps creates conditions where psychological distress often goes untreated until crisis points are reached.
In western Kenya, especially Kisumu, Siaya, and surrounding counties, localised studies have reported significantly higher rates, in some instances reaching approximately 14 per 100,000.
This region is widely identified as a mental health stress hotspot.
Interpersonal conflicts, poverty, grief, illness, and economic instability are frequently cited triggers.
Social cohesion challenges and limited access to mental health infrastructure further compound the situation, making prevention and early intervention difficult.
Urban centres present a different but equally concerning pattern.
In Nairobi, suicide cases are heavily concentrated in informal settlements and low-income neighbourhoods.
While the city may not always rank highest per capita, it contributes a large number of absolute cases due to its high population density.
Urban stressors such as unemployment, rising living costs, debt burdens, overcrowding, relationship breakdowns, and social isolation play a significant role.
The fast pace of urban life, combined with weak community ties in informal settlements, creates an environment in which emotional distress can go unnoticed until it escalates.
In central Kenya, including counties such as Kiambu, Nyeri, Murang’a, and Kirinyaga, rising concern has also been reported in recent years.
In places like Kiambu, increasing cases have been linked to drug and substance abuse, land disputes, financial stress, and social changes brought about by rapid urbanisation.
The transition from rural to peri-urban lifestyles has introduced new pressures, especially among young people struggling with employment and identity expectations in changing economic environments.
In the Rift Valley and parts of eastern Kenya, available data remains inconsistent.
This inconsistency does not necessarily indicate a lower prevalence; rather, it reflects significant underreporting and limited surveillance systems.
In these regions, poverty, alcohol use, drought-related stress, and social isolation remain important contributing factors.
The lack of consistent mental health reporting structures means many cases likely go undocumented or are attributed to other causes.
Economic hardship and mental health remain key drivers
Across all regions, despite differences in reporting and context, a clear set of shared drivers emerges.
Economic hardship remains one of the most powerful risk factors, with unemployment, debt, and poverty creating sustained psychological pressure over time.
Alcohol and substance abuse significantly increase vulnerability, particularly among men who may lack alternative coping mechanisms.
Relationship breakdowns, family conflict, academic pressure, and untreated mental health conditions such as depression and anxiety further intensify risk across all age groups.
Among young people, new and evolving pressures are also becoming more visible.
Academic expectations, social comparison driven by digital platforms, peer influence, and exposure to idealised lifestyles online contribute to feelings of inadequacy and emotional distress.
In many cases, these pressures are compounded by limited access to counselling services in schools and communities, leaving emotional struggles unaddressed.
Kenya faces a silent but deepening crisis
Ultimately, suicide in Kenya reflects a society under multiple layers of strain — economic, social, psychological, and structural.
It is a crisis that disproportionately affects young people and men, while also revealing deep regional inequalities in mental health outcomes and service access.
The clustering of cases in specific regions such as western Kenya, coastal areas, and urban informal settlements highlights how geography and inequality intersect to shape vulnerability.
While Kenya’s national suicide rate may appear lower than global averages, this figure must be interpreted with caution.
Underreporting, stigma, and uneven access to mental health care suggest that the real scale of the problem is more severe than official data reflects.
What is unfolding is a silent but deepening public health emergency continuing to grow beneath the surface of national statistics.
Addressing this crisis requires more than awareness.
READ ALSO: Tragic as Turkana teacher commits suicide after alleged aviator loss
It demands stronger national prevention systems, improved data collection and classification of deaths, expansion of mental health services across counties, integration of counselling into schools and workplaces, and community-based interventions that reach vulnerable populations early.
Without such measures, the pressures driving suicide will continue to accumulate in silence.
Kenya’s suicide landscape is therefore not only a medical or psychological issue, but also a reflection of broader social and economic realities.
It is a mirror of inequality, stress, and unmet emotional needs across generations.
Breaking the silence around it remains the first step toward meaningful change.
By Hillary Muhalya
You can also follow our social media pages on Twitter: Education News KE and Facebook: Education News Newspaper for timely updates.
>>> Click here to stay up-to-date with trending regional stories
>>> Click here to read more informed opinions on the country’s education landscape


